It's not "all in your head."
“I think it’s all in her head.” A new person assigned to my clinic team, Tim, casually told me after leaving a patient’s room.
If this were a comedy, you would see me spit out my coffee, jump out of my chair, and cover Tim’s mouth with my hand.
But this was not funny.
“We do NOT talk like that about patients anymore, especially if you’d like to work on my team,” I said sternly, which I rarely do.

This Tweet became widely popular. But what I didn’t post was the rest of the conversation.
“Oh…we don’t? Since when?” Tim asked, almost…innocently.
Since we stopped using the terms “neurasthenia” or “wandering womb” to describe any ill-health that had ever happened to a woman CENTURIES AGO? But I didn’t say that. It wouldn’t have been helpful to be sarcastic about it.
I took a deep breath, instead.
It occurred to me that what was really happening was that Tim didn’t believe the patient’s symptoms were real.
In recent years, I’ve thought about, studied, and asked about what it meant to believe the patient on my platforms. And if I have learned anything, it’s that “lecturing” someone about it won’t teach them.
I had to find another way to answer Tim’s question.
We are bad at believing patients. (Really, really bad.)
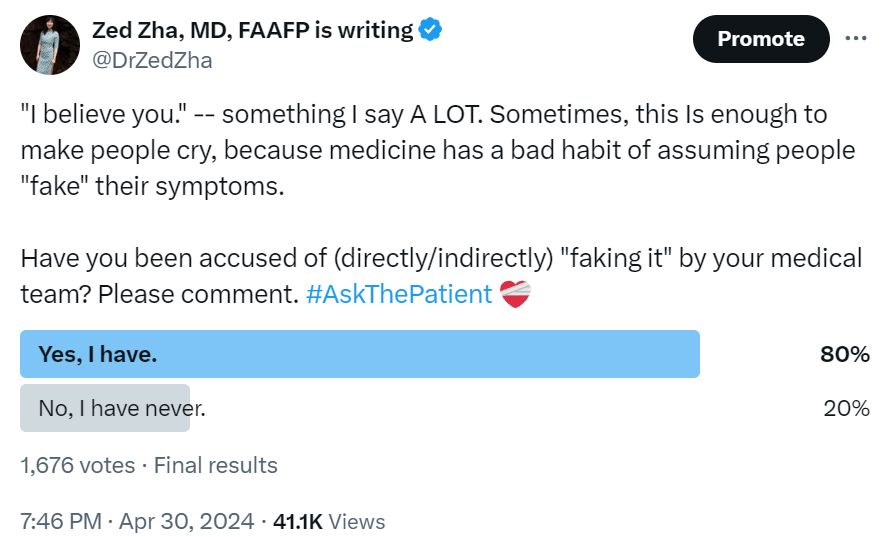
Recently, I asked the #AskThePatient community if they’ve ever felt accused of “faking” their physical symptoms. 1,676 voted, and 80% answered “yes”! Specifically, Among the hundreds of comments, many said their symptoms were chalked up to “anxiety,” “stress,” “childhood trauma,” or even “unconscious guilt for never having had a baby…”
“It’s all in your head” isn’t comedy indeed, it’s reality.
What does it actually mean to “believe someone?”
The English phrase “to believe someone” means “to credit someone with value,” or “to accept the words of someone as sufficient evidence of the truth.” Sounds simple, right? But in Chinese, my mother tongue, the phrase “to believe”, 相信, actually translates into “to put faith in each other.”
In other words, believing someone is not a one-way street. And neither is medicine.
Suddenly, the formula gets complicated. Again, I turned to the #AskThePatient community to teach me more. And here is what they (you) said:

Believing the patient is the BARE MINIMUM of healthcare.
In fact, it’s the bare minimum of any human care.
“To believe me is to see me as an equal human being.”
“Believing me is only the prerequisite. The absence of it = the denial of care.”
Worse yet, the absence of believing the patient can make someone lose faith in the healthcare system completely, as ironically put in this comment:
“To be believed is to be a…thin, white man whose symptoms fit the textbooks perfectly. Just kidding…to be believed as a patient is to be dreaming…”
(While I acknowledge the intersectionalities of medical gaslighting, medical misogyny, and medical racism, they are beyond the scope of today’s newsletter.)
So…what should believing the patient LOOK LIKE?
When it comes down to it, there are some actionable items.
“To listen to me actively and empathetically.”
“To acknowledge my symptoms, experiences, and concerns.”
“To take the appropriate and prompt actions and do what is necessary in my care.”
But these are not enough.
To truly show that we believe the patient, as my ancestors defined “相信” — we must actively involve the person in front of us.
Welcome to the two-way relationship called “believing the patient.”
“To have my input integrated into the diagnostic and treatment process.”
“To stop saying ‘I’ and start saying ‘we.’”
Actually…believing the patient is more than just words or actions. It is deeply emotional. Because to patients, to be believed FEELS LIKE…
“Having my rights, dignity, and autonomy respected.”
“No longer struggling alone but as part of a team.”
“Being validated that I am knowledgable about my own body.”
To put it simply, being believed literally equals…
“Being taken seriously.”
“Being allowed to return to my body.” And
“Being heard.”
When patients SEE that they are believed and FEEL believed, something wonderful happens!
Some might even say it’s THE thing that every young, bright-eyed medical student dreams of doing one day. Because when patients are believed, they…
“Have hope (again).”
“Can just be a patient. I don’t have to advocate for myself constantly or stress over my next appointment with the doctor every single time.”
Imagine a world where patients can be unburdened with the task of convincing doctors to believe them, where they can be just patients, whose only job is to get better. That’s when they…
“Can finally begin to heal.”
To heal.
Isn’t that what we all set out to do as doctors?
“Come with me,” I said to Tim.
Without boring the readers, the visit went like this: Tim and I went back to the patient’s room. I expressed my concerns when I saw the patient’s full-body rash and how she was scratching herself silly. I examined her entire body both with my hands and dermascope. I took photos. When she was dressing back up, Tim and I stepped out to study her recent medication changes with the pharmacist. Then we went back to look at the photos she saved on her phone, thanked her for keeping such thorough documentation, and took photos of her photos. I told her my theories of what might be going on. Then I offered a biopsy and explained why. I was open about my reasoning and told her that I would be OK with skipping the biopsy and trying some treatments without it. We decided to do the biopsy. After, I gave her the treatments I thought were most likely going to work. One of them was a pill.
“This medication is to help you with itching. It works in the brain, that’s why it has the side effects it has.” I paused briefly. “But I am not saying, by any means, that this is all in your head.”
By the time these words came out, it felt silly.
“Oh. Pff. I know that.” The patient laughed.
Later that day, I hosted a group session with my psychologist colleague for women who suffered from Hidradenitis Suppurativa (HS) — a chronic, inflammatory skin condition that results in recurrent, painful sores in private areas. I asked Tim to help.
“Who here has been told that, somehow, YOU are to blame for your HS?” I asked.
People living with HS often have been told that they had this condition because they were too fat, too dirty, too stressed, or wore jeans too tight for their bodies, etc.
Everyone raised their hands.
“And who here has felt that you were completely ALONE in your suffering?”
A woman bursted into tears quietly. Another’s eyes welled up.
Everyone raised their hands, again.
Then I saw someone walk from the corner of the room next to the crying patient, put one hand on the patient’s shoulder, and use the other to wipe away his own tears.
That was Tim, my new team member.
Disclaimers:
The above stories are based on real events but the details (including names) have been significantly altered to protect everyone’s confidentiality. The quotes are either directly from the #AskThePatient polls or paraphrased. And finally, my medical teams are made of incredibly caring people, without whose support I wouldn’t be able to do what I do. The lesson to believe the patient was one I had to learn the “hard way” myself, and arguably, still learning each and every day. This newsletter isn’t to shame anyone but to make the point that we can ALL continue to look within and improve.
Thank you for reading. I hope you feel heard. More importantly, I hope you feel believed. Please consider supporting my work by subscribing or sharing this post!